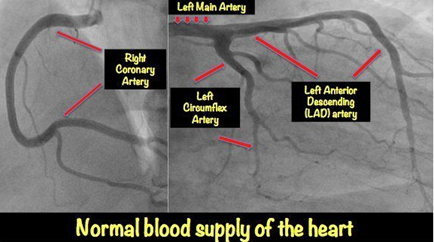
A 76-year-old man presents to your Monday morning following repeated episodes of substernal chest pain over the weekend, which the patient though was indigestion from drinking 4 glasses of wine. He has a history hypertension, hyperlipidaemia, and type 2 diabetes mellitus was admitted to the hospital for a diverticular bleed two years ago. You suspect a cardiac cause and send him to the hospital. After initial evaluation, he undergoes a cardiac catheterization which reveals severe coronary artery disease, including 70% stenosis of the left main coronary artery, 90% stenosis of the proximal left anterior descending artery, and 80% stenosis of the right coronary artery. Given the severity of his disease, antiplatelet agents are discontinued, and he is started on a heparin drip in preparation for coronary artery bypass surgery the following day.
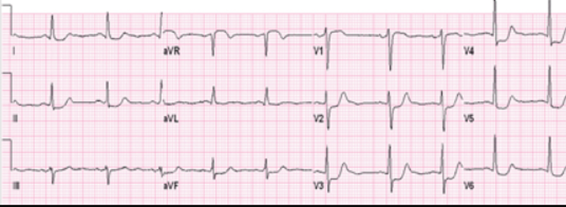
Five hours after catheterization, he develops sudden hypotension (BP 75/60 mmHg) and tachycardia (120/min). He reports generalized weakness and back pain but denies chest pain, dyspnoea, nausea, or abdominal discomfort. On examination, he appears diaphoretic and clammy, with flat neck veins. Heart sounds are normal, and the chest is clear to auscultation. The right groin puncture site is mildly tender but without swelling or bruit. After receiving 1000 mL of normal saline, his blood pressure improves to 96/60 mmHg, and his pulse decreases to 85/min. His repeat ECG is unchanged.
Q: Which of the following is the most appropriate next step in managing this patient?
Learning Objective
Retroperitoneal hematoma is a known complication of cardiac catheterization, particularly when the femoral artery is accessed above the inguinal ligament. It often presents with sudden hypotension, tachycardia, back pain, and hemodynamic instability without visible external bleeding. Diagnosis is confirmed with a non-contrast CT scan of the abdomen and pelvis, and management is supportive with IV fluids, blood transfusion as needed, and hemodynamic monitoring.
Most Appropriate Next Step
✅ Non-contrast CT scan of the abdomen and pelvis
This patient’s presentation is highly suggestive of a retroperitoneal hematoma, a known complication of cardiac catheterization, especially when performed via the femoral artery. The sudden onset of hypotension, tachycardia, flat neck veins, back pain, and clinical improvement with IV fluids strongly indicate internal bleeding rather than cardiogenic shock. If the arterial puncture site is above the inguinal ligament, the hematoma may extend into the retroperitoneal space with minimal visible signs externally. Diagnosis is best confirmed with a non-contrast CT scan of the abdomen and pelvis or, alternatively, an abdominal ultrasound if CT is unavailable. Management is typically supportive, involving IV fluids, blood transfusion as needed, and close monitoring.
In the case of suspected retroperitoneal hematoma following cardiac catheterization, a non-contrast CT scan of the abdomen and pelvis is preferred because:
- Detection of Acute Haemorrhage:
- Fresh blood appears as hyperdense (bright) on non-contrast CT, making it easy to identify hematoma formation.
- Contrast is not necessary for visualizing a hematoma because it does not provide additional information about the bleeding itself.
- Avoiding Confounding Enhancement:
- If contrast is used, it may obscure the hematoma by enhancing nearby vascular structures, making it harder to distinguish the extent of the bleed.
- Avoiding Nephrotoxicity in High-Risk Patients:
- The patient has diabetes and hypertension, both of which increase the risk of contrast-induced nephropathy (CIN).
- Given that he is hemodynamically unstable, reducing the risk of kidney injury is a priority.
- Quick and Readily Available:
- A non-contrast CT is faster and more widely available, allowing for rapid diagnosis without the delays of contrast administration.
When Would Contrast Be Used?
- If active bleeding is suspected and the goal is to identify an ongoing vascular source, CT angiography (contrast-enhanced CT) may be used. However, in this case, the clinical scenario suggests a contained hematoma rather than ongoing arterial bleeding.
Incorrect Answer Choices
❌ CT scan of the chest with contrast
A CT scan of the chest with contrast is used to diagnose acute aortic dissection, which typically presents with sudden, tearing chest pain radiating to the back, pulse deficits, or mediastinal widening on chest X-ray. Aortic dissection following cardiac catheterization is extremely rare and usually occurs in the right coronary sinus due to catheter-induced trauma. This patient’s symptoms (flat neck veins, back pain, and hemodynamic instability) suggest a retroperitoneal bleed rather than aortic dissection.
❌ Nasogastric tube placement
Nasogastric tube (NGT) placement can be useful in evaluating upper gastrointestinal bleeding by detecting fresh blood or “coffee ground” material. However, this patient has no symptoms of GI bleeding (e.g., hematemesis, melena, or hemodynamic instability unrelated to recent cardiac procedures). His history of diverticular bleeding is not relevant to his acute presentation. Furthermore, his symptoms (back pain and flat neck veins) point toward a vascular complication rather than an upper GI source.
❌ Stat transthoracic echocardiogram (TTE)
A transthoracic echocardiogram is useful for diagnosing pericardial effusion and cardiac tamponade, which present with jugular venous distension, muffled heart sounds, pulsus paradoxus, and an enlarged cardiac silhouette on imaging. However, this patient has flat neck veins rather than distended ones, making cardiac tamponade unlikely. Additionally, tamponade from cardiac procedures typically follows pericardiocentesis or coronary perforation, neither of which occurred here.
❌ Proceeding with urgent coronary artery bypass grafting (CABG)
While CABG is necessary for this patient’s severe coronary artery disease, performing urgent surgery in the setting of active bleeding would be dangerous. His hypotension is likely due to haemorrhage rather than cardiac ischemia, and surgery could worsen his clinical status due to increased blood loss and hemodynamic instability. The priority is to diagnose and stabilize the bleeding first.
References
- Australian cardiovascular intervention guidelines
- Australian Journal of General Practice – Vascular Complications of Cardiac Catheterization
- Medical Journal of Australia – Managing Post-Catheterization Bleeding